Distinguishing between razor burn and herpes simplex virus infections presents a common diagnostic challenge that affects millions of individuals worldwide. Both conditions can manifest as painful, red lesions in sensitive areas of the body, particularly around the genital region, leading to considerable anxiety and confusion. The ability to accurately differentiate between these conditions is crucial not only for appropriate treatment selection but also for understanding transmission risks and long-term health implications.
Recent dermatological studies indicate that approximately 45% of individuals who experience genital skin irritation initially misidentify their condition, with razor burn being mistaken for herpes in roughly 30% of cases. This diagnostic uncertainty stems from overlapping symptoms and similar anatomical distributions, making professional medical evaluation essential for definitive diagnosis. Understanding the distinct characteristics of each condition empowers individuals to make informed decisions about when to seek medical attention and what treatment approaches may be most appropriate.
Understanding razor burn: clinical manifestations and pathophysiology
Razor burn represents a multifaceted inflammatory skin condition that encompasses several distinct pathophysiological processes. This common dermatological issue affects an estimated 78% of individuals who engage in regular shaving practices, with severity ranging from mild irritation to significant inflammatory responses requiring medical intervention. The condition typically develops through mechanical trauma to the skin surface, disrupting the protective barrier function and triggering localised inflammatory cascades.
The primary mechanism underlying razor burn involves the interaction between sharp blade edges and delicate skin structures. During the shaving process, microscopic abrasions occur along hair follicles and surrounding epithelial tissues, creating entry points for irritants and potential bacterial colonisation. These micro-injuries activate inflammatory mediators including histamine, prostaglandins, and various cytokines, resulting in the characteristic erythema, swelling, and discomfort associated with razor burn.
Folliculitis and Post-Shaving inflammatory response mechanisms
Folliculitis represents one of the most common complications associated with razor burn, occurring when hair follicles become inflamed or infected following shaving trauma. This condition manifests as small, red, pimple-like bumps surrounding individual hair follicles, often accompanied by mild to moderate discomfort and localised swelling. The inflammatory response typically peaks within 24 to 48 hours post-shaving, with symptoms gradually subsiding over the following week.
The pathogenesis of post-shaving folliculitis involves disruption of the follicular epithelium, allowing normal skin flora, particularly Staphylococcus epidermidis and Propionibacterium acnes , to penetrate deeper tissue layers. This bacterial infiltration triggers an innate immune response characterised by neutrophil recruitment, complement activation, and the release of inflammatory mediators. The resulting inflammatory milieu creates the characteristic papular eruption pattern observed in follicular razor burn.
Pseudofolliculitis barbae: ingrown hair complications
Pseudofolliculitis barbae, commonly referred to as ingrown hair syndrome, represents a chronic inflammatory condition that disproportionately affects individuals with curly or coarse hair textures. This condition occurs when recently shaved hairs re-enter the skin surface at an angle, creating a foreign body reaction that results in persistent inflammatory papules and eventual scarring if left untreated. Research indicates that up to 83% of Black males experience some degree of pseudofolliculitis barbae, highlighting the significant ethnic predisposition associated with this condition.
The clinical presentation of pseudofolliculitis barbae differs markedly from acute razor burn, featuring chronic, recurring inflammatory lesions that persist long after the initial shaving event. These lesions often develop a characteristic appearance, with visible curved hairs beneath the skin surface and surrounding hyperpigmentation. The condition typically worsens with repeated shaving, creating a cycle of inflammation and tissue damage that can result in permanent scarring and keloid formation in susceptible individuals.
Contact dermatitis from shaving products and metal sensitivity
Contact dermatitis represents another important component of the razor burn spectrum, involving allergic or irritant reactions to shaving products, razor blade materials, or topical preparations used during the grooming process. Allergic contact dermatitis typically develops 24 to 72 hours after exposure to sensitising agents, while irritant contact dermatitis manifests more rapidly, often within minutes to hours of product application.
Common allergens implicated in shaving-related contact dermatitis include fragrance compounds in shaving creams, preservatives such as formaldehyde-releasing agents, and nickel present in razor blade alloys. The clinical presentation often extends beyond the immediate shaving area, creating broader patterns of erythema, vesiculation, and scaling that can help differentiate this condition from other forms of razor burn. Patch testing may be necessary to identify specific allergens and guide future product selection.
Temporal progression of razor burn symptoms within 24-48 hours
The temporal evolution of razor burn symptoms follows a predictable pattern that aids in differential diagnosis and treatment planning. Initial symptoms typically appear within minutes to hours of shaving, beginning with mild erythema and progressing to more pronounced inflammation over the subsequent 12 to 24 hours. Peak symptom intensity generally occurs between 24 and 48 hours post-shaving, after which gradual resolution begins in uncomplicated cases.
Early-stage razor burn presents as diffuse erythema with possible mild oedema, often accompanied by a burning or stinging sensation. As the inflammatory process progresses, discrete papular lesions may develop, particularly in areas of follicular involvement. By 48 to 72 hours, symptoms typically begin to subside, with complete resolution expected within one week in most cases. Persistent symptoms beyond this timeframe warrant consideration of alternative diagnoses or complicating factors such as secondary bacterial infection.
Herpes simplex virus: HSV-1 and HSV-2 diagnostic characteristics
Herpes simplex virus infections represent one of the most prevalent sexually transmitted infections globally, with the World Health Organisation estimating that 3.7 billion people under age 50 carry HSV-1 and 491 million people aged 15-49 have HSV-2 infections. These viral pathogens establish lifelong latent infections within nerve ganglia, periodically reactivating to produce characteristic vesicular eruptions on skin and mucous membranes. The ability to distinguish between HSV-1 and HSV-2 infections has become increasingly important as treatment protocols and transmission counselling strategies continue to evolve.
HSV-1 traditionally causes orofacial herpes, manifesting as cold sores or fever blisters around the mouth and lips, though genital HSV-1 infections have increased dramatically over the past two decades. HSV-2 primarily affects the genital and perianal regions, causing recurrent painful vesicular eruptions with varying frequency and severity. Both viral types share similar replication cycles and clinical presentations, though HSV-2 typically demonstrates higher recurrence rates and more severe symptomatology, particularly during primary infections.
Vesicular eruption patterns in primary herpes outbreaks
Primary herpes simplex virus infections present with distinctive vesicular eruption patterns that differ significantly from razor burn manifestations. These initial outbreaks typically begin as clusters of small, fluid-filled vesicles measuring 1-3 millimetres in diameter, arising on an erythematous base. The vesicles contain clear, serous fluid that becomes increasingly turbid as viral replication progresses and inflammatory cells accumulate within the lesion.
The distribution pattern of primary herpes lesions follows anatomical nerve pathways, creating characteristic grouped vesicular arrangements that rarely occur in razor burn cases. Primary genital herpes often presents bilaterally, affecting multiple anatomical sites within the same dermatome, including the external genitalia, perineum, and upper thighs. This extensive distribution pattern, combined with severe systemic symptoms, helps distinguish primary herpes from localised razor burn reactions.
Prodromal symptoms: tingling, burning, and neuralgic pain
One of the most distinguishing features of herpes simplex virus infections involves the presence of prodromal symptoms that precede visible lesion development by 6 to 48 hours. These neurological symptoms result from viral replication within sensory nerve ganglia and the subsequent inflammatory response affecting nerve function. Patients commonly report tingling, burning, or shooting pain sensations in areas where lesions will subsequently appear, often describing these sensations as distinctly different from typical skin irritation.
The neuralgic quality of herpes prodromal symptoms provides a crucial diagnostic clue that distinguishes viral infections from razor burn. While razor burn may cause burning or stinging sensations, these symptoms typically correlate directly with visible skin irritation and lack the deep, neurological quality characteristic of herpes prodromal phases. Additionally, herpes prodromal symptoms often occur in individuals with no recent shaving history, further supporting viral aetiology over mechanical trauma.
Viral shedding timeline and lesion evolution stages
The evolution of herpes simplex virus lesions follows a predictable timeline that provides important diagnostic and therapeutic implications. Viral shedding begins during the prodromal phase and peaks during the vesicular stage, typically lasting 7-12 days in primary infections and 3-5 days in recurrent episodes. Understanding this timeline is crucial for both accurate diagnosis and transmission risk assessment.
The lesion progression typically follows five distinct stages: prodromal symptoms, vesicle formation, ulceration, crusting, and healing. Vesicles usually rupture within 24-48 hours, creating shallow, painful ulcerations with irregular borders. These ulcers subsequently develop yellow-brown crusts as epithelial repair processes begin. Complete healing, including crust separation and epithelialisation, typically requires 7-14 days for primary infections and 5-10 days for recurrent episodes.
Recurrent episode manifestations and decreased severity patterns
Recurrent herpes simplex virus infections demonstrate markedly different clinical patterns compared to primary episodes, with reduced symptom severity, shorter duration, and more localised lesion distribution. These differences result from established immune memory responses that limit viral replication and tissue damage. Recurrent episodes typically present as smaller clusters of vesicles, often numbering fewer than ten lesions, compared to the extensive eruptions characteristic of primary infections.
The frequency of recurrent episodes varies significantly between individuals and viral types, with HSV-2 generally causing more frequent recurrences than HSV-1. Studies indicate that individuals with genital HSV-2 experience an average of 4-6 recurrences annually during the first year following primary infection, with frequency typically decreasing over time. This recurrent pattern represents a key distinguishing feature from razor burn, which occurs only following mechanical trauma and does not demonstrate spontaneous recurrence.
Anatomical distribution differences between razor burn and herpes
The anatomical distribution of lesions provides one of the most reliable methods for distinguishing between razor burn and herpes simplex virus infections. Razor burn demonstrates a precise correlation with areas of recent hair removal, creating linear or geometric patterns that correspond to razor blade trajectories. These patterns typically appear as parallel lines or rectangular areas of inflammation, particularly evident in regions where multiple razor passes occurred or where shaving technique was suboptimal.
In contrast, herpes simplex virus lesions follow neuroanatomical distributions that correspond to specific dermatomes and nerve pathways. Genital herpes typically affects the S2-S4 dermatomes, creating lesion clusters that may extend from the external genitalia to the buttocks, posterior thighs, and perianal region. This distribution pattern bears no relationship to hair removal practices and often includes areas that are never shaved, such as the inner aspects of the labia or the coronal sulcus of the penis.
The bilateral nature of many herpes outbreaks provides another distinguishing feature, as viral replication within nerve ganglia can affect multiple anatomical sites simultaneously. Primary genital herpes commonly presents with lesions on both sides of the midline, affecting structures such as the bilateral labia majora, bilateral buttocks, or bilateral thighs. Razor burn, conversely, typically demonstrates unilateral predominance corresponding to hand dominance and shaving technique patterns.
Facial involvement patterns also differ significantly between these conditions. Herpes labialis characteristically affects the vermillion border of the lips and adjacent facial skin, areas that are rarely involved in typical male facial shaving routines. When herpes affects the beard area, lesions often extend beyond the typical shaving zone to include the ears, neck, or forehead, following trigeminal nerve distributions rather than grooming patterns.
Morphological analysis: lesion appearance and textural variations
Detailed morphological analysis of individual lesions provides critical diagnostic information for differentiating razor burn from herpes simplex virus infections. This analysis encompasses lesion size, shape, colour, texture, and internal contents, each providing specific clues regarding underlying pathophysiology. Professional healthcare providers rely heavily on these morphological characteristics when making clinical diagnoses, particularly in cases where patient history or anatomical distribution patterns remain ambiguous.
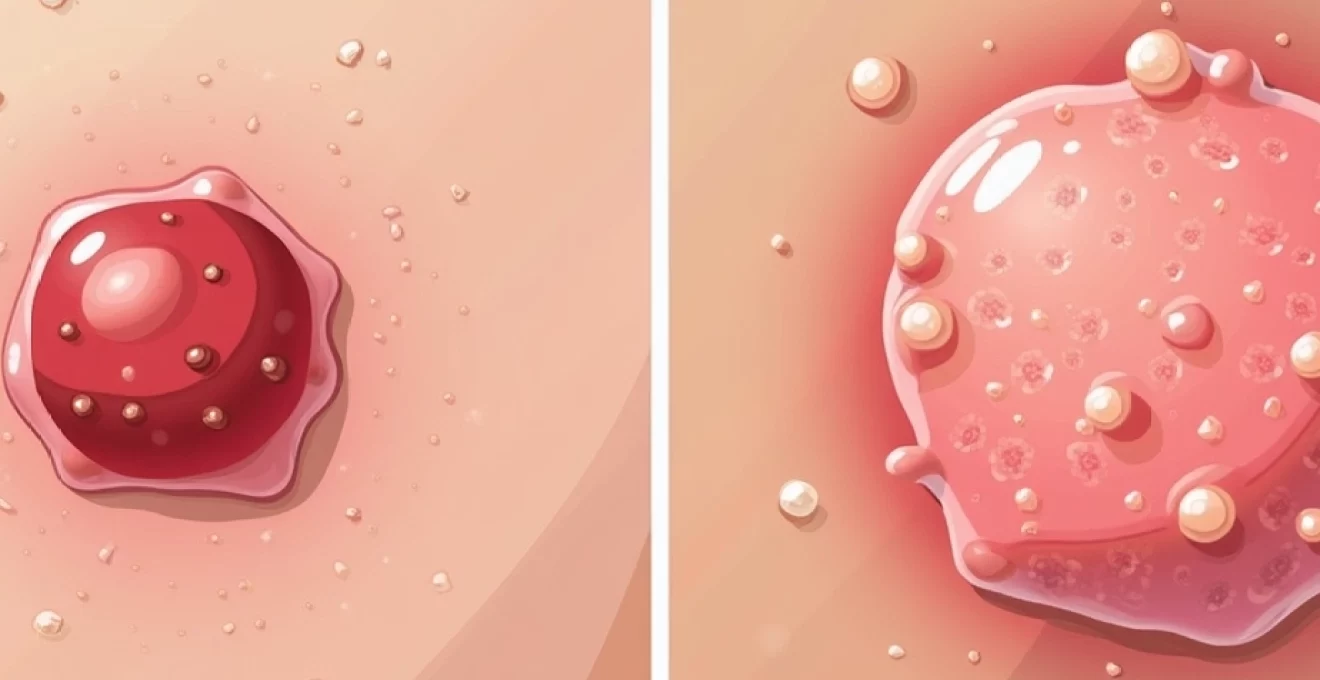
Erythematous papules versus Fluid-Filled vesicles
The fundamental difference between razor burn and herpes lesions lies in their basic morphological structure and formation mechanisms. Razor burn primarily manifests as erythematous papules, representing solid elevations of skin resulting from inflammatory infiltration and oedema within the dermis. These papules typically measure 1-5 millimetres in diameter, exhibit a firm consistency on palpation, and maintain their structural integrity throughout the healing process.
Herpes vesicles, in contrast, represent fluid-filled cavities within the epidermis or at the dermal-epidermal junction, created by viral cytolysis and inflammatory exudate accumulation. Fresh herpes vesicles appear as translucent, dome-shaped elevations with clearly visible fluid contents, ranging from clear to slightly opalescent depending on inflammatory cell concentration. The vesicular nature of herpes lesions makes them particularly fragile, often rupturing spontaneously or with minimal trauma.
Examination techniques for distinguishing papules from vesicles include gentle palpation to assess lesion consistency and the use of oblique lighting to highlight surface characteristics. Papular razor burn lesions feel firm and maintain their shape under light pressure, while vesicular herpes lesions demonstrate fluctuance and may rupture during examination. The presence of visible fluid within lesions strongly suggests viral aetiology rather than mechanical irritation.
Crusting patterns and ulceration characteristics
The development of crusting and ulceration provides additional morphological markers for differential diagnosis between razor burn and herpes infections. Razor burn lesions rarely progress to ulceration unless complicated by secondary bacterial infection or excessive mechanical trauma. When crusting occurs in razor burn cases, it typically represents dried inflammatory exudate or small amounts of serous fluid, creating thin, easily removable crusts that do not indicate significant tissue destruction.
Herpes ulceration follows vesicle rupture and represents true epithelial loss, creating shallow, well-demarcated ulcers with characteristic “punched-out” appearances. These ulcerations typically measure 2-8 millimetres in diameter and exhibit irregular, slightly raised borders with surrounding erythema. The ulcer base often appears red and granular, indicating active epithelial repair processes, and may demonstrate a yellowish fibrinous coating in deeper lesions.
The crusting patterns associated with healing herpes ulcers differ markedly from razor burn presentations. Herpes crusts tend to be thick, adherent, and honey-coloured, representing dried viral exudate combined with inflammatory debris and healing epithelial tissue. These crusts often persist for several days and leave temporary hyperpigmentation following separation, while razor burn crusts typically resolve more rapidly without significant colour changes.
Healing progression: epithelialisation versus viral resolution
The healing progression patterns of razor burn and herpes lesions reflect their distinct underlying pathophysiological mechanisms and provide valuable diagnostic information throughout the recovery period. Razor burn healing follows typical wound repair processes, with inflammatory resolution occurring within 24-48 hours and complete epithelial restoration within 3-7 days. This healing progression demonstrates steady improvement without the fluctuating symptom patterns characteristic of viral infections.
Herpes lesion healing involves complex interactions between viral clearance, immune system activation, and epithelial regeneration. The healing timeline typically extends over 7-14 days for primary infections and 5-10 days for recurrent episodes, with distinct phases including vesicle formation, ulceration, crusting, and epithelialisation. Unlike razor burn, herpes healing may demonstrate temporary worsening during the ulcerative phase before improvement begins.
Residual changes following healing also differ between these conditions. Razor burn typically resolves completely without permanent tissue alterations, though temporary hyperpigmentation may occur in individuals with darker skin types. Herpes healing may leave subtle
scarring patterns, including areas of hypopigmentation or hyperpigmentation that may persist for weeks to months. These post-inflammatory changes provide retrospective diagnostic clues and may indicate previous viral infections in patients with unclear clinical presentations.
Laboratory testing methods: PCR, viral culture, and serology
Laboratory testing represents the gold standard for definitive diagnosis when clinical presentations remain ambiguous or when accurate identification is crucial for patient management and partner counselling. Modern diagnostic methods have evolved significantly over the past decade, offering improved sensitivity, specificity, and turnaround times compared to traditional testing approaches. The selection of appropriate testing methods depends on lesion characteristics, timing of presentation, and specific clinical objectives.
Polymerase chain reaction (PCR) testing has emerged as the preferred diagnostic method for active herpes simplex virus infections, demonstrating sensitivity rates exceeding 95% when performed on appropriate specimens. This molecular technique amplifies viral DNA sequences, allowing detection of even minimal viral loads present in clinical specimens. PCR testing can differentiate between HSV-1 and HSV-2 infections, providing crucial information for prognosis and transmission counselling. The test requires collection of vesicular fluid, ulcer exudate, or tissue samples from active lesions, making timing of specimen collection critical for optimal results.
Viral culture methods, while less sensitive than PCR, remain valuable for certain clinical scenarios and research applications. Culture techniques involve inoculating clinical specimens onto susceptible cell lines and monitoring for characteristic cytopathic effects over 2-7 days. This method allows for viral isolation and subsequent antiviral sensitivity testing, which may be important in cases of suspected drug resistance. However, culture sensitivity decreases significantly as lesions heal, with optimal results obtained from fresh vesicular specimens collected within 48 hours of lesion onset.
Serological testing utilises type-specific assays to detect HSV-1 and HSV-2 antibodies, providing information about previous viral exposure and immune status. Type-specific serology can identify asymptomatic infections and help clarify infection history in patients with unclear clinical presentations. However, serological testing cannot distinguish between active and latent infections and may not detect recent infections due to the window period required for antibody development. Results interpretation requires careful consideration of clinical context and testing limitations.
Direct fluorescent antibody testing and antigen detection methods offer rapid diagnostic options for clinical settings requiring immediate results. These techniques can provide results within hours but demonstrate lower sensitivity compared to PCR methods, particularly for healing lesions or specimens with low viral loads. The choice between immediate versus delayed testing depends on clinical urgency, available resources, and the potential impact of results on patient management decisions.
Professional medical consultation: when to seek dermatological assessment
Professional medical consultation becomes essential when clinical presentations deviate from typical razor burn patterns or when diagnostic uncertainty creates anxiety or inappropriate self-treatment attempts. Healthcare providers possess the clinical expertise and diagnostic tools necessary to accurately differentiate between various causes of genital skin irritation, ensuring appropriate treatment and preventing potential complications. The decision to seek professional evaluation should consider both immediate symptom severity and broader health implications of accurate diagnosis.
Urgent medical evaluation is warranted when lesions demonstrate rapid progression, extensive distribution, or severe associated symptoms such as fever, malaise, or significant pain. Primary herpes infections, in particular, can present with dramatic symptomatology requiring prompt antiviral intervention to minimise symptom duration and severity. Additionally, lesions that persist beyond expected healing timeframes or demonstrate unusual characteristics warrant professional assessment to exclude alternative diagnoses or complications.
Individuals with compromised immune systems face heightened risks from both delayed diagnosis and inappropriate treatment, making professional consultation particularly crucial for this population. Conditions such as HIV infection, diabetes mellitus, immunosuppressive medications, or autoimmune disorders can alter typical disease presentations and healing patterns. These patients may experience atypical lesion morphology, prolonged healing times, or increased complication rates that require specialised management approaches.
Sexual health considerations provide another compelling reason for professional evaluation, particularly when herpes infection is suspected. Accurate diagnosis enables appropriate partner notification, transmission risk counselling, and implementation of prevention strategies. Healthcare providers can discuss suppressive therapy options, safer sex practices, and the psychological aspects of sexually transmitted infection management. This comprehensive approach addresses both immediate medical needs and long-term relationship and mental health considerations.
Pregnant individuals require immediate medical evaluation for any genital lesions due to the potential risks of maternal-fetal transmission during delivery. Herpes simplex virus infections during pregnancy necessitate careful monitoring and may require modifications to delivery planning to prevent neonatal transmission. Even lesions that appear consistent with razor burn should be evaluated professionally in pregnant patients to ensure accurate diagnosis and appropriate obstetric management.
Recurrent lesion patterns that develop without clear precipitating factors such as recent shaving warrant professional investigation to determine underlying causes. While recurrent razor burn can occur in individuals with persistent poor shaving techniques or product sensitivities, spontaneous recurrence of lesions often suggests viral infections or other dermatological conditions requiring specific treatment approaches. Healthcare providers can establish monitoring protocols and develop management strategies tailored to individual patient needs and symptom patterns.
The availability of telehealth consultations has expanded access to professional medical evaluation, particularly beneficial for individuals experiencing anxiety about genital symptoms or those in geographic areas with limited dermatological services. Virtual consultations allow for initial assessment, photographic documentation review, and guidance regarding the need for in-person examination or laboratory testing. This approach can provide reassurance for benign conditions while identifying cases requiring urgent intervention or specialised care.